Features

On World Malaria Day 2023, the global fight against malaria has hit a critical point in Africa. Recent studies have confirmed that malaria parasites resistant to artemisinin have emerged in Rwanda, Uganda and the Horn of Africa.
Artemisinin-based combination therapies (ACTs) are the first line treatment for malaria and there is no immediate replacement available. The loss of ACTs will put millions of Africans, mostly children under the age of 5, at risk of drug-resistant malaria infection and death.
One possible solution?
Adding a third drug to current ACT drug combinations. These Triple ACTs or TACTs have been found in clinical trials in Asia to be highly efficacious even in places where ACTs were failing.
'It is so much easier to prevent antimalarial drug resistance than to try and contain it. We are in danger losing of our current antimalarial drugs to resistance,' said Professor Sir Nick White, University of Oxford Professor of Tropical Medicine based at the Mahidol-Oxford Tropical Medicine Research Unit (MORU), in Bangkok.
'Triple artemisinin combination treatments [TACTs] will protect against resistance and help ensure that these drugs remain effective until new drugs arrive in 5-10 years time,' said Professor White.
Before TACTs can be widely deployed in Africa, however, their efficacy, safety and tolerability must be confirmed in African populations, especially children.
To that end, the Development of Triple Artemisinin-based Combination Therapies (DeTACT) trial is studying in eight African and two Asian countries two new TACTs - Artemether+lumefantrine+amodiaquine and Artesunate+piperaquine+mefloquine - to generate evidence that they are safe and effective malaria therapies.
The DeTACT project has also conducted modelling, ethics and market positioning studies to support their use in Africa and thereby prevent or delay the emergence of artemisinin and multi-drug resistant malaria.
'The DeTACT project aims to provide the necessary evidence that TACTs can both delay antimalarial drug resistance to existing drugs, and be an effective treatment for multidrug resistant infections. DeTACT will also deliver a product to market, and engage with national and global policy makers and stakeholders to discuss the potential position of TACTs in the mix of antimalarial drugs,' said University of Oxford Professor Arjen Dondorp, DeTACT project Principal Investigator.
Led by University of Oxford-affiliated researchers based at MORU in Bangkok, and funded by UK Aid administered through the Foreign, Commonwealth and Development Office (FCDO), the DeTACT trial has recruited over ~1800 patients as of April 2023 , with recruitment and follow-up completed in Niger and Nigeria, and no major or unexpected safety signals detected.
Once recruitment and follow-up are completed at the end of 2023, DeTACT investigators will present results in April 2024. Prior to that, they aim to present interim findings at a DeTACT symposium in October 2023 at the American Society of Tropical Medicine and Hygiene (ASTMH) 72nd Annual Meeting in Chicago, USA.
The first modelling study to project the impact of TACTs in preventing or delaying artemisinin resistance, led by Associate Professor Ricardo Aguas, University of Oxford, and Associate Professor Maciej Boni, Pennsylvania State University, has been completed and will soon be published in the prestigious journal, Nature Communications.
'These DeTACT modelling studies and market positioning studies generate data that will be crucial in our efforts to effectively introduce TACTS and to project the impact and cost-effectiveness of TACTs in preventing the spread of artemisinin resistance. Along with the clinical trial, these studies constitute a comprehensive assessment of the expected advantages and potential barriers to the large-scale use of TACTs,' explained Dr Chanaki Amaratunga, DeTACT Project Coordinator.
The DeTACT project has engaged malaria stakeholder engagement officers to communicate directly with National Malaria Control Programmes (NMCPs) to present to them to the DeTACT project and TACTs in general. Presentations on DeTACT and TACTs have been made at the RBM Partnership to End Malaria Case Management Working Group and the Seasonal Malaria Chemoprevention (SMC) Alliance Annual meetings. These efforts have led to significant interest from all parties in participating in future research and exploring the roll-out of TACTs in their countries.
To make TACTs available as quickly as possible where they are most needed it is critical to work with the pharmaceutical industry on the co-formulation. MORU has signed a memorandum of understanding with Fosun Pharma, China, and the Medicines for Malaria Venture (MMV) to develop and pre-qualify fixed-dose combinations of artemether-lumefantrine-amodiaquine, prior to deploying them across Africa.
'The DeTACT trial will generate data not only on the efficacy and safety of TACTs but also on the pharmacokinetics of each of the drug components, including in malnourished children – a particularly vulnerable sub-population. In addition, there will be cutting-edge analyses, combining clinical trial data with that from whole genome and transcriptome studies, to improve our understanding of artemisinin and antimalarial drug resistance,' said Dr Mehul Dhorda, DeTACT-Africa Coordinator.
Further reading
Market Formation in a Global Health Transition.
Triple Artemisinin-Based Combination Therapies for Malaria - A New Paradigm?

Tatjana Gibbons, a DPhil student at Oxford’s Nuffield Department of Women's & Reproductive Health, talks about research to develop a new 20-minute diagnostic test for endometriosis.
Around one in ten women will develop some form of endometriosis in their lives, a disease that affects more than 190 million women worldwide.
Yet despite its common occurrence, it typically takes eight years for a diagnosis – a figure that has shown no sign of improving in the past decade. The problem is that it typically involves several visits to the GP and hospital referrals, multiple scans and often surgery to diagnose.
Not only does this leave patients suffering for a significant period of time, but it can also require unpleasant and invasive procedures.
Aside from the pain, discomfort and worry about an ongoing undiagnosed condition, an important issue is its effect on fertility when left unchecked. A national questionnaire we conducted with over 1000 respondents with confirmed or suspected endometriosis found that 88% of respondents had experienced a delay in diagnosis, and 72% felt that an earlier diagnosis would have changed their life choices with regard to decisions such as fertility planning. With earlier diagnosis, it is possible to treat both the pain and discomfort as well as to begin to consider fertility options such as freezing eggs for the future.
The problem with diagnosing endometriosis is that small lesions in the pelvis are not detected on ultrasound and often need surgery to detect. This is why we are assessing alternative ways of looking inside the body without being invasive.
Our research group is conducting the DETECT (Detecting Endometriosis expressed inTEgrins using teChneTium-99m) imaging study, to investigate whether an experimental image marker (⁹⁹ᵐTc-maraciclatide) that binds to areas of inflammation can be used to visualise endometriosis using a 20-minute scan. In endometriosis, small parts of the lining of the uterus – the endometrium – are found in the fallopian tubes, ovaries or in the pelvis (for example, attached to bowel). The presence of the endometrium outside of the uterus leads to inflammation in the pelvis, which this test will aim to highlight.
If this is successful, it will give us a fast and effective way to identify any case of endometriosis, as well as assessing how serious the patient’s individual condition is and may even be able to distinguish between old and new disease.
Professor Christian Becker, who is Co-Director of the Endometriosis CaRe Centre in Oxford together with Professor Krina Zondervan, Head of Department at the Nuffield Department of Women’s and Reproductive Health, University of Oxford, will lead this initial study on women due to have planned surgery for suspected endometriosis.
Two to seven days before their operation, the participants will be invited for an imaging scan which will compare the suspected locations of disease detected on the scan and in surgery to confirm whether this imaging test matches what is found.
The beauty of this approach is that, if successful, it will provide a quick, painless and affordable option for tens of millions of women worldwide.
To read more about this research project and the partners involved, please visit https://www.wrh.ox.ac.uk/news/new-imaging-study-could-make-diagnosing-endometriosis-quicker-more-accurate-and-reduce-the-need-for-invasive-surgery
The study is being carried out in partnership with Serac Healthcare, a UK-based developer of breakthrough imaging technology.

By Dr Louise Dalton and Dr Elizabeth Rapa of Oxford's Department of Psychiatry.
Every day, thousands of parents and grandparents are diagnosed with serious health conditions such as cancer, lung or heart disease. They are then faced with the unenviable task of sharing this information with the children they love.
Research has shown that effective communication with children about parental illness has long term benefits for children and their family’s physical and mental health. These include better child psychological well-being, as well as lower reported symptoms of depression, anxiety and behavioural problems. It also has benefits for parental mental health, adherence to treatment (such as following the prescribed drug regime) and family functioning.
However, adults find sharing a diagnosis with children one of the most difficult experiences. Understandably, they want to protect children from distress and many feel uncertain about whether children need to be told, or when and how to navigate these sensitive conversations. Yet, children are “astute observers” and are often acutely aware of changes within the family. Silence about what is happening risks children misinterpreting the situation and worrying alone, without access to the emotional support they need.
Previous research has found that patients want help from their clinical team to think about what, how and when to share their diagnosis with children, or how to answer questions such as “Are you going to die?” – but often report finding this support difficult to find. However, few studies have asked healthcare professionals about how they perceive their role regarding the needs of patients’ wider families. A team from the Department of Psychiatry interviewed 24 NHS clinicians from different professional backgrounds and working across a range of specialties to find out more about their views and experiences regarding the needs of patients’ children.
Our latest study, published in PLOS One, found that although patient’s family details were often recorded, this information was not routinely used to help patients share their diagnosis with children. In other situations, patients’ relationships with children were rarely or never identified.
The NHS healthcare professionals who took part reported feeling uncertain about asking patients about what children understand. They feared that they would make the situation worse or upset their patients.
“What can I say, what if they are in pieces, what do I do with that at that time of day? It seems a bit crass to enquire about something you aren’t in a position to help with.” GP
“Your worst fear is saying the wrong thing” Oncology
It was also frequently assumed that someone else in the clinical team would talk to the patient about their children, but often this meant opportunities for these conversations were missed.
“How that is dealt with, I am not really in the loop. […] So you don’t really know what happens to those children in terms of who says what to them. Someone might, but not me.” Surgery
Because you are talking to them [adult patient] directly, you tend to leave it to them to approach that [talking to their children]. Not that that is necessarily right, but it is the way it tends to happen.”
Others recognised their vital role and the importance of “thinking about the children and the family as whole” and being honest about the reality of the patient's situation.
“Don’t ever tell your child an untruth, don’t say ‘It’s all going to be fine, I am going to live forever’. Be truthful.” Neurology
While acknowledging the multiple demands on healthcare teams, the authors recommend a culture shift in recognising that talking to children about their parent's illness improves family relationships and mental health. Sharing patients’ desire for support from their clinical team around these issues may reassure healthcare professionals that initiating a conversation about children will be welcomed. Indeed, clinicians can play a key part in reassuring and guiding families to open up this sensitive topic with children. Working in partnership, healthcare professionals and families can protect the psychological well-being of children who are affected by the illness of an adult they love.
This is an important area to get right and a programme of research led by Dr Louise Dalton, Dr Elizabeth Rapa and Professor Alan Stein focusses on facilitating family centred conversations with clinical teams in every discipline. The team are currently developing a resource for all healthcare professionals to help them identify children who are important to their adult patients irrespective regardless of their patients’ diagnosis or age. This will be freely available to everyone and show professionals how four short steps during a consultation could have huge benefits for their patients and loved ones, with a lasting legacy for children’s psychological wellbeing.
The study, 'Exploring healthcare professionals’ beliefs, experiences and opinions of family-centred conversations when a parent has a serious illness: A qualitative study', can be read in PLOS One.

By Maria Czepiel, who has recently submitted her doctorate and is a stipendiary lecturer at Brasenose and Balliol colleges. Her DPhil was in the Faculty of Medieval and Modern Languages and funded by the Open-Oxford-Cambridge Doctoral Training Partnership.
Garcilaso de la Vega (1501-1536), Spain’s greatest Renaissance poet, was in equal parts man of action and bard: as he writes in one of his poems, his life consisted of taking up ‘now the sword, now the pen’ (‘ora la espada, ora la pluma’).
He was part of the court of the Habsburg king and Holy Roman Emperor Charles V, and took part in battles and campaigns in Europe and North Africa. However, his career was not without hiccups; in 1532, he was condemned to exile by the king for having participated in the wedding of his nephew (which did not have the king’s approval). He spent some months confined to an island on the Danube near Ratisbon, before being sent to Naples in the service of the Spanish viceroy. In the years that followed, he reported to the king on various sensitive political and diplomatic issues, which seems to have earned him back the monarch’s good graces. He died of wounds received in battle in 1536.
While I was studying for my DPhil, I came across a 16th century printed book of Latin poetry...I was excited to find previously unidentified copies of the three Latin odes by Garcilaso.
As a poet, he is particularly famous for introducing classical and Italian forms such as eclogues, elegies and odes into Spanish poetry. As well as writing in Spanish, in his day, Garcilaso was also praised for his poetry in Latin. Unfortunately, until recently only three of his Latin odes were extant. We also knew, from a letter by the Italian humanist and poet Pietro Bembo, that Garcilaso had dedicated an ode to him, and that Bembo was especially pleased by it, but no copies of it survived.
While I was studying for my DPhil, I came across
 A statue of the renowned Garcilaso de la Vega in his home town of Toledo.
Credit: Shutterstock
A statue of the renowned Garcilaso de la Vega in his home town of Toledo.
Credit: ShutterstockIn his ode to the Italian, Garcilaso modestly claims he is not a very good poet, but that if he were, he would use his gifts to extol Bembo. He then goes on to do exactly that and praise Bembo’s poetry and work as an historian of Venice. Part of the aim of Garcilaso’s poem must have been to gain the approval of the older poet, which would admit him into the most elite literary circles of the period. (The strategy worked: Bembo wrote back to Garcilaso saying that he not only exceeded all Spanish poets, but even gave the Italians a run for their money.)
I was even more excited to notice the poems were followed by two more poems attributed to Garcilaso, and one of them was the poem dedicated to Bembo which had been lost for almost 500 years
The second poem is addressed to a German poet called Johann Alexander Brassicanus, who was not previously known to have a connection with Garcilaso. The poem describes tents and armies on the banks of the Danube, which suggests it refers to the period of exile. Until now, we have only had negative impressions of Garcilaso’s time in Germany, when he says he was ‘imprisoned […] in a foreign land’ (‘preso […] en tierra ajena’) and separated from his wife and family.
Now we have a more positive view, since in this poem Garcilaso speaks warmly of a friendship he made during that time: Brassicanus is ‘Among the first of my companions, bonded | To Lassus by undissolvable law | To the end of my life’ (‘sodalibus | In primis habite, indissociabili | Lasso lege revincte | Vitae tempora ad ultima’, 1–4). In short, these two poems give us new insights both into Garcilaso’s aspirations as a poet, as well as into parts of his fascinating life as a man of action.
I wrote an article about my discovery which has just come out in the Bulletin of Spanish Studies (https://www.tandfonline.com/doi/full/10.1080/14753820.2022.2122386). I hope the find will stimulate more interest in Garcilaso’s life and Latin poetry, and perhaps more odes will turn up when we least expect it.
Dr Qiang Zhang of the Radcliffe Department of Medicine explains how artificial intelligence is being used to help researchers and physicians interpret medical imaging.
Disruptive AI-based imaging technology might replace the injection of dye ‘contrast agents’ usually needed to show clear images of scar of the heart
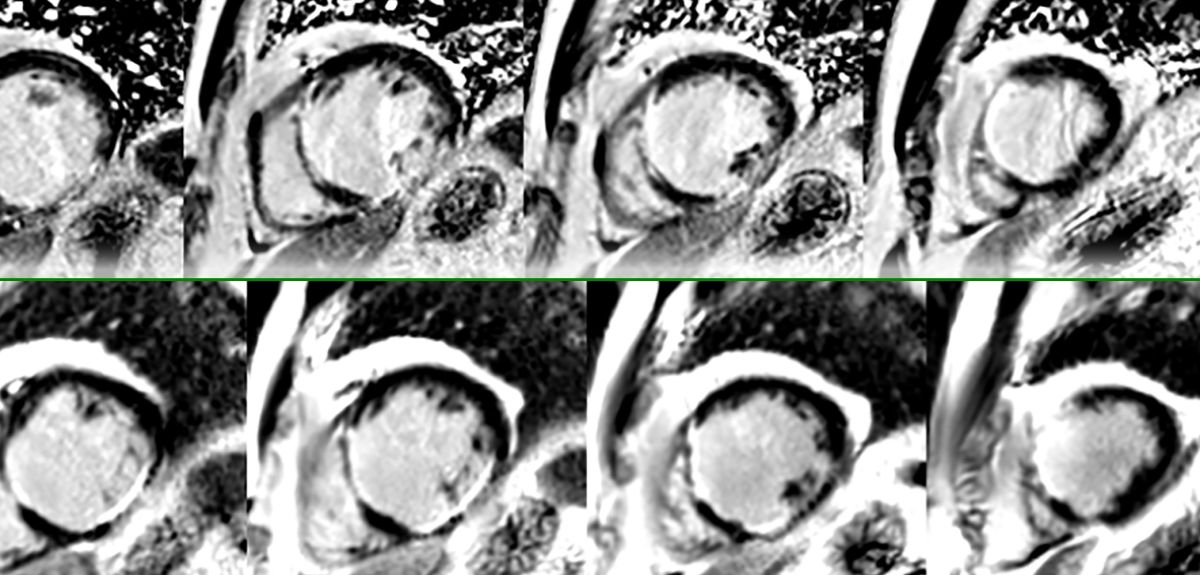
Imagine you are a medical doctor, faced with a patient with suspected heart disease for symptoms such as chest pain, tightness, or shortness of breath. One way to find out what is happening, and help guide patient prognosis, is to do a cardiovascular MRI scan to look into any heart muscle abnormalities. The scan involves injecting a ‘contrast agent’ (a dye that will improve image contrast and show up scars on images) into a vein in the patient. Contrast-enhanced MRI has been the clinical standard to provide clear scar images, but it’s painful, and makes already expensive MRI scans even more so.
What’s more, this method is limited in patients with significant kidney failure – their kidneys have difficulty clearing the dye from their bodies, sometimes leading to irreversible complications. Some patients will be allergic to the contrast agent, and you might want to limit the use of injectable contrasts in some patients, such as pregnant women and children.
So how do you find out about what might be going on in your patient’s heart in that case, without injecting into them a contrast agent?
It turns out that injecting a contrast agent might not be the only way to get clear MR images to reveal scars in the heart muscle – in 2010, Professor Stefan Piechnik from the Radcliffe Department of Medicine at Oxford University came up with a method to study heart muscle properties, using a contrast-free MRI technique called T1-mapping. It produces an image of the heart with numerical values that change with different diseases.
Such contrast-free MRI contain a lot of information about heart tissue properties, some of which is subtle, or difficult to identify as a scar or other pathologies. As of now, researchers are still exploring the best ways to interpret and display the information from these contrast-free T1-maps, which is one of the reasons that they are not yet widely used by medical doctors.
This is why our cross-disciplinary team of AI scientists, magnetic resonance imaging specialists and cardiologists at the University of Oxford worked to find ways that artificial intelligence (AI) can enhance these contrast-free MRIs, to produce clear images of heart muscle scarring. AI effectively works like “virtual contrasts” to replace conventional intravenous contrasts.
We developed an AI-powered algorithm to combine multiple contrast-free MR images together with heart motion information, enhance the pathological signals in them, to reveal scars in a similar way to conventional contrast-enhanced MRI. This technology is called “virtual native enhancement”, or VNE, as it acts as an enhancer for the MR images, using only the ‘native’ (ie, non contrast agent enhanced) images produced by an MRI scanner.
In 2021, our team released the first proof of concept for this idea, by detecting scars in the heart muscle for patients with hypertrophic cardiomyopathy, a common genetic heart disease affecting 1 in 500 people, and the most common cause of cardiac death among young people.
Recently, we have found that VNE can also detect scars in patients who have had a heart attack. We compared contrast-free VNE with conventional contrast-enhanced MRI in these patients. We found that VNE highly agreed with the conventional MRI in detecting previous heart attack scars and their extent. Additionally, the VNE image quality was actually better, all without the patients needing to receive an injection.
Once completely validated, this new technology may slash the time that patients need to spend in an MRI scanner from the standard 30-45 minutes to within 15 minutes, saving more than half the scan cost, yet producing images that are clearer, more diagnostically useful, and easier to interpret.
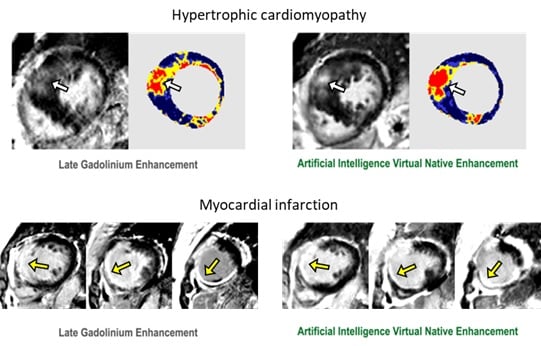
Image: Development of VNE in detecting heart muscle scars for two different heart diseases. The right panels show our new contrast-free method, while the left panels show conventional contrast-enhanced which requires injecting contrast agents. Arrows point to the detected scars.
We think that these successive breakthroughs mark the beginning of a new era of diagnostic medical imaging, using AI instead of IV contrasts to reveal pathologies in the human body: we might finally be able to get rid of injections when it comes to heart MR imaging.
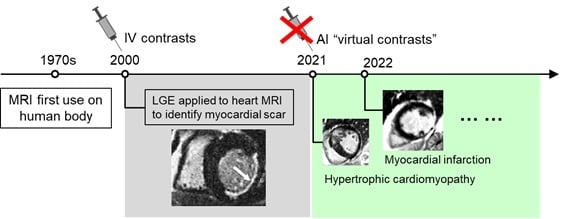
Image: Background of IV contrasts of MRI, and the emerging new era of AI “virtual contrasts”.
We are now working to further improve the capabilities of this technology, to detect more complex heart diseases and their underlying mechanisms, beyond the diagnostic power of current MRI. We plan to use these methods in large clinical studies as a diagnostic tool for novel investigations.
We think that this kind of Virtual Native Enhancement technology is an exciting and potentially game-changing advance for clinical MRIs in the future. Patients going in for a clinical MRI scan might not need an injection for most MRI scans, not just for the heart, but potentially for other organs as well. This would cut costs for healthcare providers, meaning that many more patients could access MRI scans; the risks of contrast-agent injections complications would disappear too. We hope adoption of this method could contribute to the digitalization of the NHS, something which is very much needed to address the backlog post COVID-19 pandemic.
With thanks to Professor Stefan Piechnik and Professor Vanessa Ferreira, joint senior authors of the study.
Further reading in Circulation: Zhang et al 2021, Zhang and Burrage et al 2022.
- ‹ previous
- 5 of 9
- next ›
 25-year Oxford study finds the effects of conflict last for generations
25-year Oxford study finds the effects of conflict last for generations What Louise Thompson’s campaign tells us about the national maternity crisis
What Louise Thompson’s campaign tells us about the national maternity crisis Celebrating 25 Years of Clarendon
Celebrating 25 Years of Clarendon  Learning for peace: global governance education at Oxford
Learning for peace: global governance education at Oxford  What US intervention could mean for displaced Venezuelans
What US intervention could mean for displaced Venezuelans  Setting the agenda for the next century of quantum
Setting the agenda for the next century of quantum 10 years on: The Oxford learning centre making an impact
10 years on: The Oxford learning centre making an impact Mapping the Moon: the world’s first lunar atlas goes digital
Mapping the Moon: the world’s first lunar atlas goes digital  Oxford and The Brilliant Club: inspiring the next generation of scholars
Oxford and The Brilliant Club: inspiring the next generation of scholars New course launched for the next generation of creative translators
New course launched for the next generation of creative translators